Why Dental Lab Quality Control Still Fails — Even After Final Inspection
A Common Scenario Most Clinics Have Experienced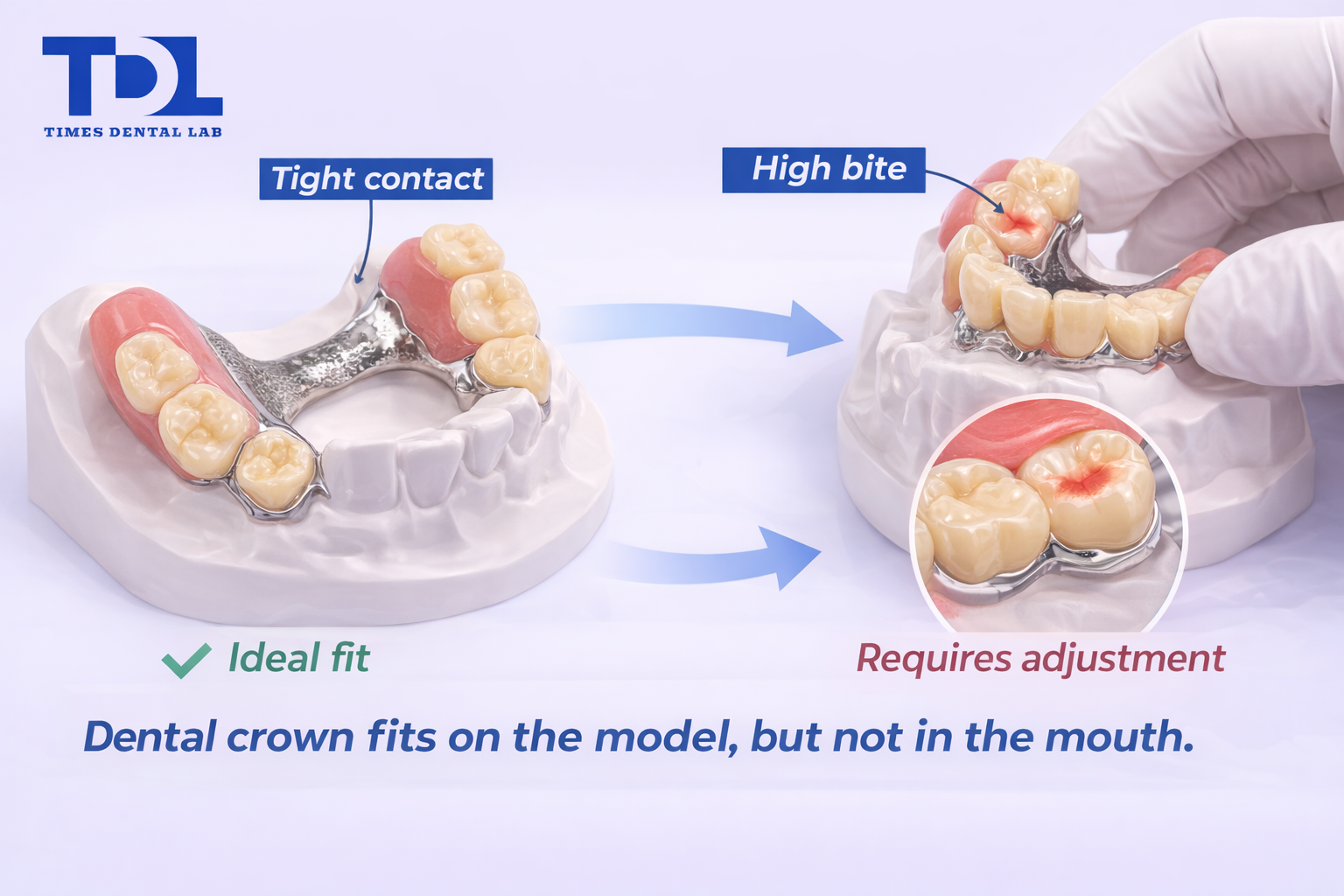
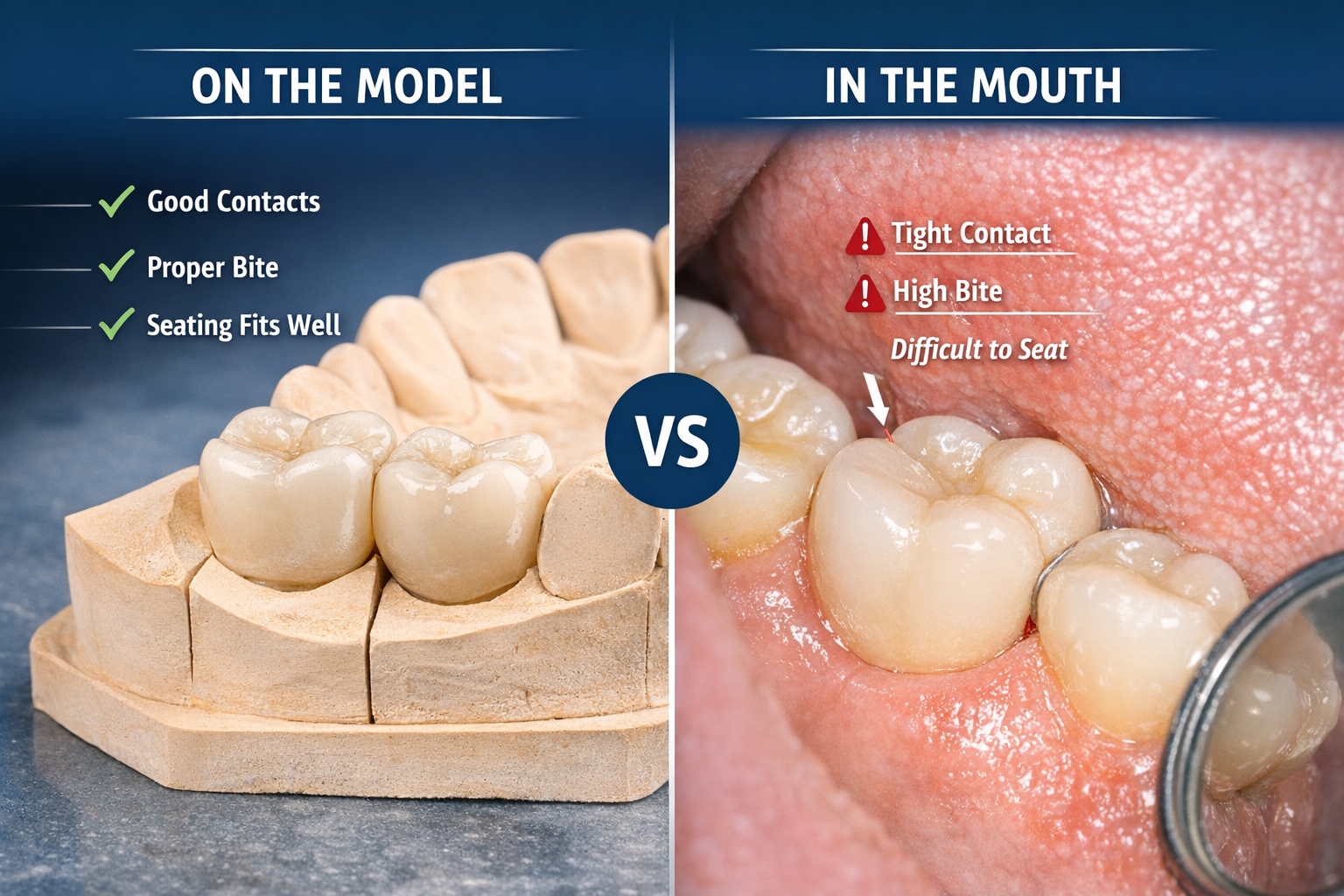
A crown passes quality control.
On the model, everything looks acceptable.Contacts feel within range.Occlusion seems stable.
But once the crown is seated in the mouth:
· The contact feels tighter than expected
· The bite is slightly high
· Adjustment is needed
Nothing is dramatically wrong.But something is not quite right.
This situation is common.And it raises an important question:
If the case passed quality control,why does it still require adjustment?
The answer is not always in the final check.
In many cases, the issue started much earlier.
What Dental Lab Quality Control Is Supposed to Do
Dental lab quality control is often understood as a final inspection step.
But in practice, its purpose is different.
Quality control is not only about identifying visible defects.It is about controlling variation — before it becomes a problem.
In crown and bridge work, this includes:
· Contact relationship
· Occlusion
· Margin integrity
· Overall fit and seating
Each of these elements has a tolerance range.
A case does not need to be perfect.But it needs to be predictable.
When quality control works properly, the result behaves as expected:
· Contacts are adjustable with minimal effort
· Occlusion requires only minor refinement
· Seating is stable and passive
The goal is not to eliminate all variation.It is to keep variation within a controllable range.
Common Misunderstandings About Quality Control

In daily communication, several assumptions about QC often appear.
They sound reasonable, but they are incomplete.
QC is the final step
In many workflows, QC is treated as the last checkpoint before delivery.
This creates a false expectation:
If the case passes QC, it should be correct.
In reality, QC at the final stage can only evaluate what has already been produced.
It cannot change earlier decisions.
QC can fix any problem
Some issues can be adjusted at the end:
· Slightly tight contact
· Minor occlusal interference
But others cannot be fully corrected:
· Incorrect bite registration
· Insufficient restorative space
· Misinterpreted margins
By the time these issues reach final QC,they are no longer easily reversible.
QC is mainly visual
Visual inspection is only one part of quality control.
Functional checks are equally important:
· Contact tension
· Occlusal balance
· Seating behavior
A crown that looks correct is not always clinically correct.
Why Final Inspection Alone Cannot Prevent Problems
Final inspection happens after key decisions have already been made.
At that stage:
· The design is fixed
· The material has been processed
· The geometry cannot be easily changed
This means:
QC at the end can detect problems,but it cannot always prevent them.
For example:
If the bite registration is inaccurate,the occlusion may appear correct on the model,but behave differently in the mouth.
If the available space is insufficient,the restoration may be adjusted to fit,but structural compromise may occur.
These are not failures of inspection.They are limitations of timing.
Where Quality Deviations Actually Start
Most deviations do not begin at the end.
They begin at earlier stages:
Case intake
· Incomplete scans
· Missing areas
· Distorted impressions
These issues introduce uncertainty from the start.
Case evaluation
During dental lab case review, decisions are made about:
· Whether the data is usable
· Whether clarification is needed
· Whether the case should proceed
Skipping this step increases downstream risk.
Design interpretation
Even with complete data, interpretation matters:
· Contact tightness preferences
· Occlusal scheme
· Margin handling
Small differences here affect final behavior.
Production execution
Material handling, finishing, and adjustmentcan introduce further variation.
What Should Be Checked in Dental Lab Quality Control

To understand QC properly, it helps to look at what is actually being evaluated.
Contact
Contacts should not be simply “tight” or “open”.
They should fall within a controllable range:
· Too tight → difficult seating
· Too open → food impaction
Occlusion
Occlusion must be assessed in relation to the provided bite.
Important factors include:
· Contact distribution
· Interference points
· Functional movement
Margin
Margin evaluation includes:
· Continuity
· Adaptation
· Extension
Even small inaccuracies can affect long-term performance.
Fit and Seating
The restoration should seat without resistance.
Indicators of poor fit include:
· Rocking
· Incomplete seating
· Uneven contact
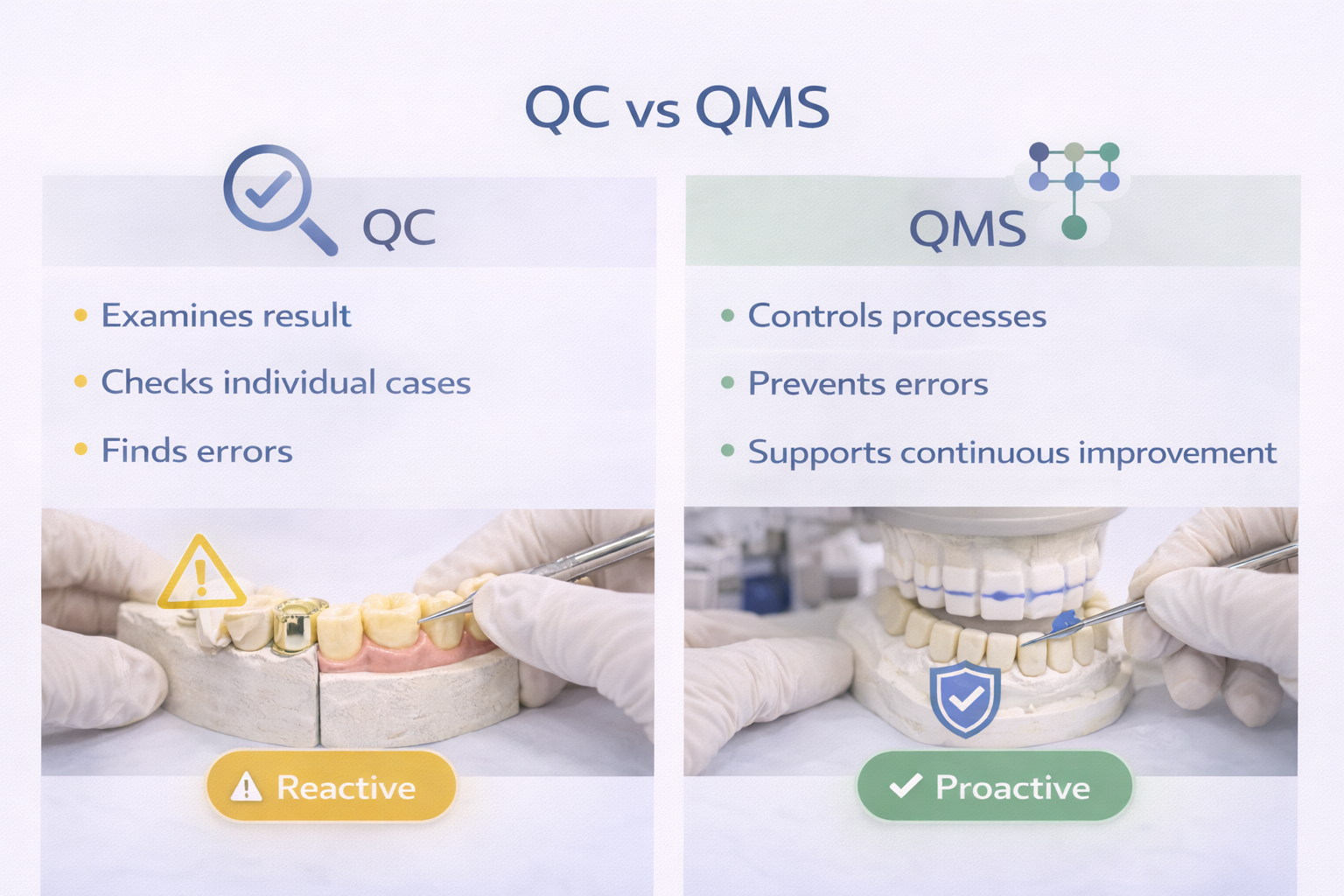
Checking vs Controlling: A Critical Difference
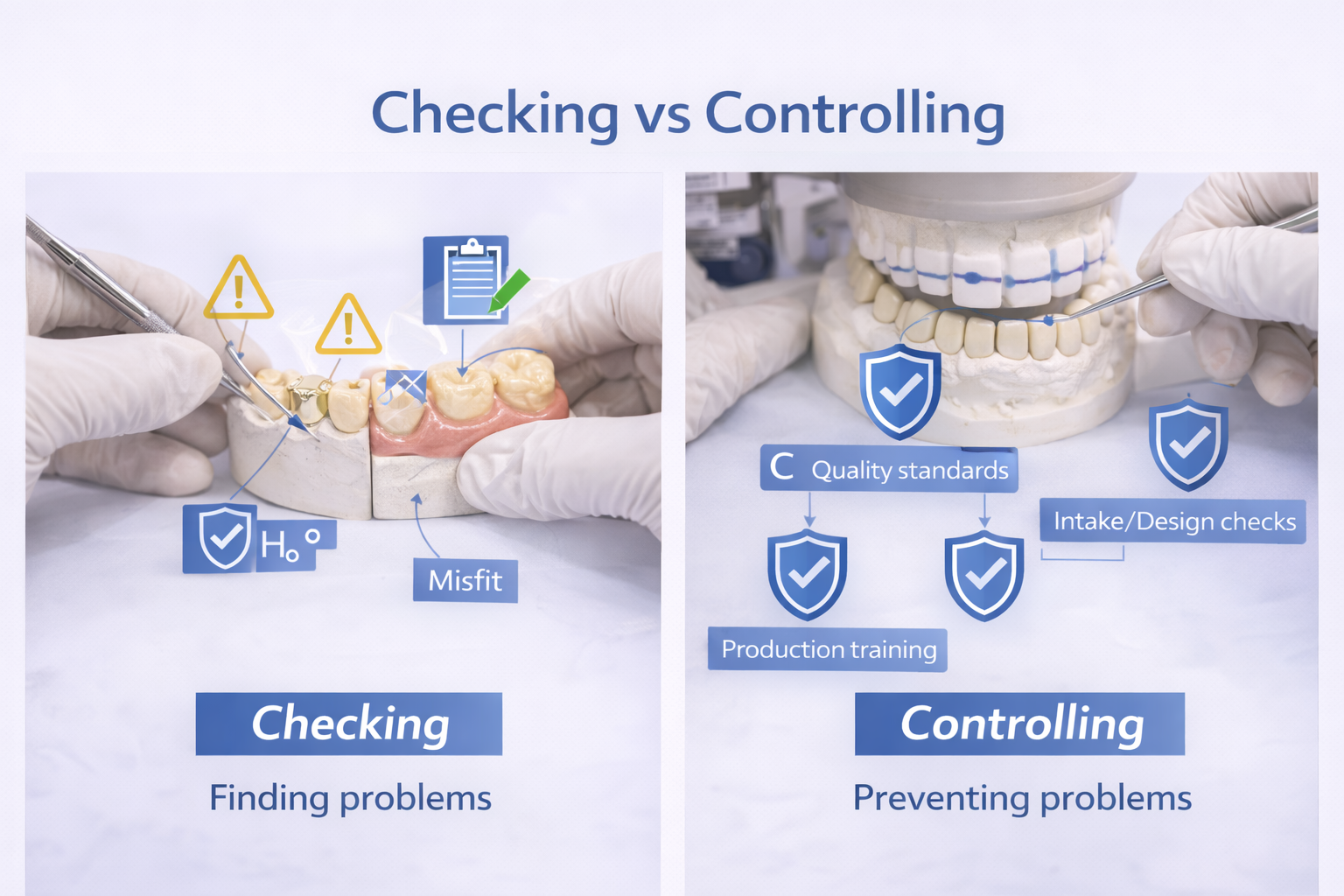
There is an important distinction between checking and controlling.
|
Checking |
Controlling |
|
Happens after production |
Happens before and during production |
|
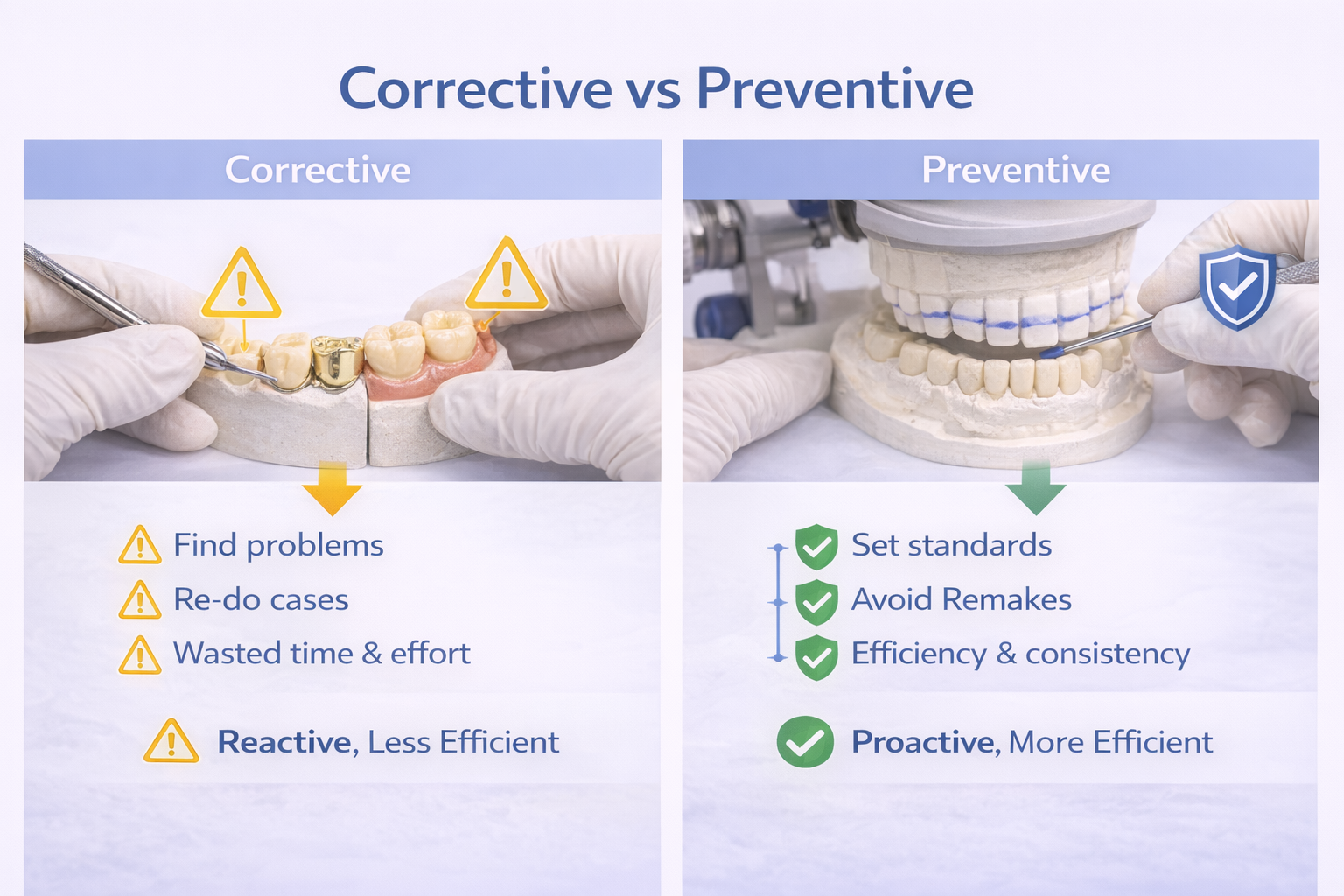
Identifies problems |
Prevents problems |
|
Reactive |
Proactive |
A workflow based only on checkingwill always be one step behind.
A workflow based on controllingreduces the chance of problems appearing at all.
Why Some Labs Have QC — But Still Feel Unstable
Many labs have a QC step.
But not all achieve consistent outcomes.
The difference lies in how QC is applied.
QC as a formality
In some workflows, QC exists but is limited to:
· Visual inspection
· Basic checks
Without integration into earlier stages,its impact is limited.
Lack of upstream control
If intake and design decisions are not standardized,variation accumulates before QC begins.
Dependence on individuals
When outcomes rely heavily on individual technicians,consistency becomes difficult to maintain.
Having QC is not enough.It must be part of a system.
How Quality Control Should Be Built Into the Workflow

Effective QC is distributed across the entire process.
Intake QC
· Verify scan completeness
· Identify missing data
· Assess bite reliability
Design QC
· Evaluate feasibility
· Confirm contact and occlusion strategy
· Identify potential risks
Production QC
· Monitor execution
· Maintain consistency in shaping and finishing
Final QC
· Verify outcome
· Confirm readiness for delivery
QC is not a step.It is a structure applied across steps.
How This Is Applied in Daily Production

In higher-volume environments, consistency depends less on individual techniqueand more on how decisions are standardized.
In daily production, it is common to encounter:
· Incomplete data
· Unclear instructions
· Variations in clinical preference
To manage this, workflows are structured to:
· Identify issues early
· Standardize decision criteria
· Apply multiple checkpoints
This approach supports more predictable outcomes,especially when handling cases across different markets and clinical expectations.
Why Consistency Matters More Than Perfection
Perfection is not always achievable in dental restorations.
Every case includes variables:
· Patient anatomy
· Bite registration
· Clinical preparation
What matters more is consistency.
Clinicians benefit from:
· Predictable contact behavior
· Stable occlusion
· Reliable seating
Consistency reduces adjustment time.It improves efficiency.
How Clinics Can Evaluate a Lab’s Quality Control System
Instead of asking whether a lab has QC,it is more useful to understand how it works.
Questions to consider:
· Is case review performed before design?
· Are issues identified and communicated early?
· Is QC applied only at the end, or throughout the process?
· Are decisions standardized or technician-dependent?
Practical indicators:
· Fewer unexpected adjustments
· More predictable fit
· Consistent outcomes across cases

Conclusion: Quality Control Is Built, Not Inspected
A crown does not fail at delivery.
It reflects decisions made throughout the process.
Small deviations — in contact, occlusion, or fit —rarely appear suddenly.
They develop over time,when something was not controlled early enough.
Quality control, in its most effective form,is not about catching errors at the end.
It is about reducing the chance of those errors appearing in the first place.